 Beyond bronchiectasis, EMBARC also conducts research into known causes of bronchiectasis – an example of which being Primary Ciliary Dyskinesia (PCD).
Beyond bronchiectasis, EMBARC also conducts research into known causes of bronchiectasis – an example of which being Primary Ciliary Dyskinesia (PCD).
EMBARC analyses clinical data from those with PCD who have been recruited into the EMBARC registry and clinical/biological sample data from those enrolled into the EMBARC-BRIDGE study to better understand the epidemiology, biology and clinical features associated with PCD.
EMBARC is also carrying out a large scale genetic study called GECCO to identify undiagnosed cases of PCD among those enrolled in the EMBARC-BRIDGE study.
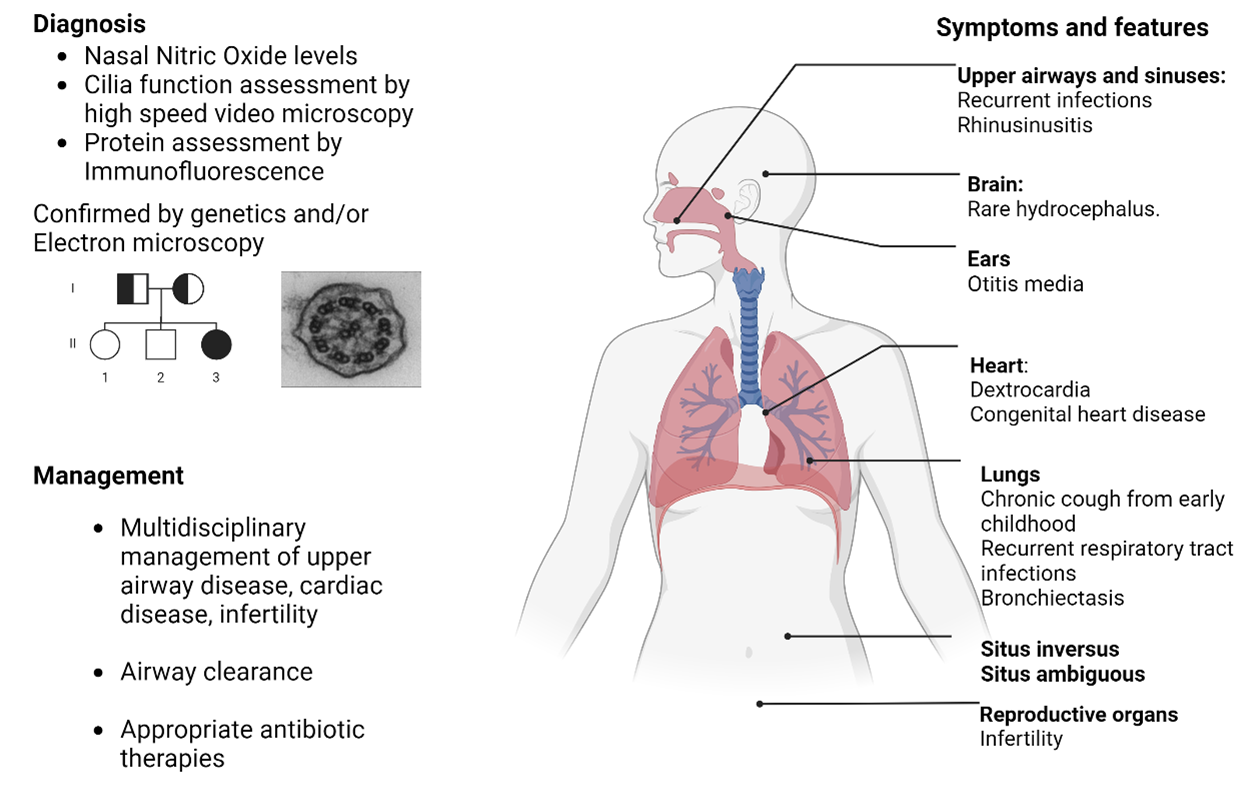
PCD often presents itself in childhood as neonatal respiratory distress and frequent respiratory infections during childhood, and the majority of patients with PCD go on to develop bronchiectasis in later life.
Cilia are present in other organs as well as the lungs and people with PCD can often present with other clinical features such as situs inversus (reversal of the organs), upper airway symptoms, or infertility.
For a diagnosis of PCD, a combination of functional and genetic tests are used. These can include taking a sample from a patients nose to look at how the cilia function, if they beat efficiently, or their structure under the microscope appears normal. A simpler test for PCD involves measuring the patient’s nasal nitric oxide, but this test cannot confirm PCD on it’s own. A diagnosis of PCD is confirmed by identification of a mutation in one (or more) of the 50 genes known to influence cilia.
The management of PCD is similar to that of other causes of bronchiectasis, with an emphasis on improving airway clearance. Additional multidisciplinary care can be required to address symptoms of other organs as well as genetic counselling where appropriate.