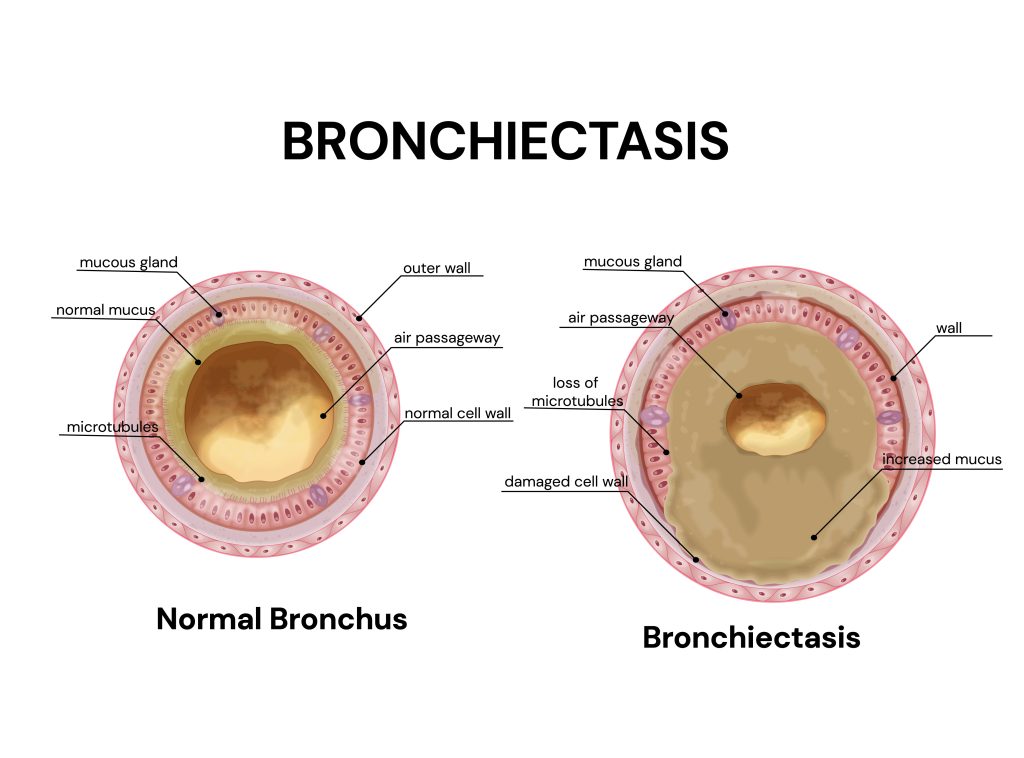
Bronchiectasis is a common, progressive respiratory disease characterised by permanent dilatation of the bronchi and presenting with a clinical syndrome of cough, sputum production and recurrent respiratory infections.
Once considered an “orphan” disease, there is growing evidence of benefit for various aspects of treatment now in bronchiectasis.
How common is bronchiectasis?
The prevalence of bronchiectasis is increasing worldwide and while estimates vary, data from a recent paper published by EMBARC in the Lancet Respiratory Medicine showed that estimates from the UK of up to 566 per 100,000 population and 174 per 100,000 from a recent study in China. The prevalence increases with age and this is likely to be a significant underestimate of the true burden of the disease. Bronchiectasis may be under-recognised and under-diagnosed; O’Brien et al studied a cohort of 110 patients with a primary care diagnosis of chronic obstructive pulmonary disease, by performing high resolution computed tomography scanning and lung function testing. They identified bronchiectasis in 29% of patients, suggesting a high prevalence of bronchiectasis among COPD patients but also suggesting a degree of mis-diagnosis as 19% of patients in this study had never smoked. Increasing awareness of the disease and improved diagnosis due to advances in computed tomography technology are likely to increase the reported prevalence.
Clinical features and impact
The most common reason for initial referral is a chronic productive cough or recurrent respiratory tract infections.Bronchiectasis is increasingly recognised as a complication of, or coincident condition with, other chronic lung disease like COPD.
Patients with mild disease may be asymptomatic, reporting symptoms only during exacerbations. The most common symptom is chronic cough, usually productive of sputum.Although “classical” bronchiectasis is associated with expectoration of purulent (dark green) sputum, patients may have muco-purulent or mucoid sputum. Sputum colour changes over time and reflects the presence of bacterial infection, often darker during exacerbations. Sputum colour can be helpfully quantified using a sputum colour chart that correlates well with patients’ symptoms, and can be reliably assessed by patients and healthcare professionals.
Less frequently, patients experience haemoptysis and pleuritic or non-pleuritic chest pain. Dyspnoea is present in around 62-74% of patients, and is most prominent in patients with severe disease. The incidence of rhinosinusitis may be as high as 80%. Patients may be systemically unwell with fatigue and malaise particularly during exacerbations.
Examination findings
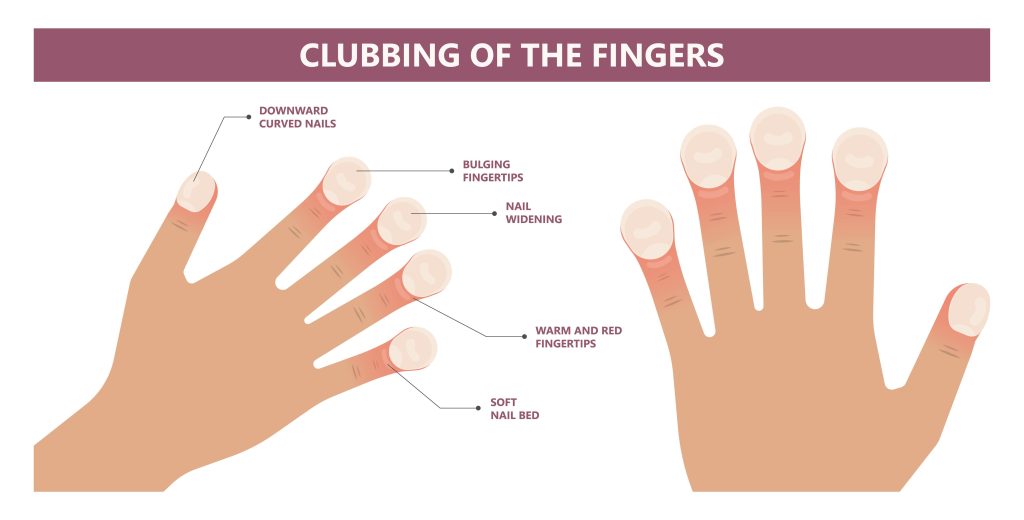
The “classical” bronchiectasis picture of finger clubbing and coarse crackles on auscultation occurs in a minority of patients with very severe disease and cystic type bronchiectasis. In practice, patients with significant bronchiectasis may have very few of these physical signs. Wheeze may occur in association with airflow obstruction and right heart failure may be seen in very severe disease.